

What is osteoporosis?
Osteoporosis is a disease with an increasing presence in society , driven by the rise in average height in recent decades and the growing life expectancy. Based on clinical data recorded by the World Health Organization (WHO), 500 million people worldwide may currently suffer from the disease, and of these, almost 3 million are in Spain alone, with associated healthcare costs exceeding 4 billion euros, according to the Spanish Society of General Practitioners and Family Physicians.
But beyond the numbers, osteoporosis is a serious health problem that affects the quality of life of those who suffer from it. A healthy, dense, and well-mineralized skeleton supports the body's weight, protects organs from impact damage, and allows for independent movement. A porous skeleton, with low mineral content, becomes fragile and brittle over time . Fractures appear in long bones, such as the femur in the hip, or in those that support more complex structures like the spine. Muscles become overloaded, nerves are compressed, joints become inflamed, and the body deforms. All of this happens slowly, sometimes over years, before the first symptoms appear.
Osteoporosis, how does it affect older people?
To understand what's behind this process, why it affects older people more, especially women past menopause , and above all what role soy plays in all this, we first need to talk a little about how the human skeleton develops and is maintained.

Human bones are essentially composed of two different and complementary parts : an organic cartilaginous matrix , mainly collagen protein fibers and other accessory fibers, which grows during childhood and adolescence until reaching the height dictated by our genetics and diet, and a rigid mineral matrix , calcium phosphate crystals with magnesium inclusions, which is deposited on it and provides structural resistance and load-bearing capacity.
Every aspect of this structure is regulated by numerous environmental, hormonal, and nutritional factors, but the engineers responsible for maintaining it are primarily two cell types integrated into the bone: osteoblasts and osteoclasts. Osteoblasts synthesize most of the components of bone, including collagen and hydroxyapatite, the crystalline form of calcium phosphate in the mineral matrix, and promote cartilage growth and mineralization (osteogenesis). Osteoclasts digest and reabsorb mineral, decreasing bone density and releasing calcium and phosphorus from the vast reserves stored in the mineral matrix when the body needs them (bone resorption). The balance in the functioning of both cell types is known as bone remodeling , and when properly regulated and nourished, it keeps the skeleton in optimal condition. However, when this balance is lost and bone resorption becomes dominant, the bone begins to lose mineral density, hardness, and strength.
That is, osteoporosis begins.
Why is this balance lost in bone remodeling?
On the one hand, the activity of osteoblasts and osteoclasts is tightly controlled by the body through hormones such as testosterone and estrogen. During puberty, the increased testosterone production in males causes osteoblasts to accelerate and osteoclasts to slow down, so that their bones grow longer and denser, on average, than those of females of the same age and weight.
Estrogens help regulate balance, and during adulthood they contribute to maintaining skeletal health . Unfortunately, menopause causes a drastic decrease in estrogen production, and bone resorption becomes dominant. Postmenopausal women and other groups with estrogen deficiency are the main risk group for osteoporosis, and there is no single therapeutic approach that covers all cases. Some hormone replacement therapies that attempt to mimic the effects of estrogens in patients, such as SERM-type estrogen modulators, estrogen agonists like raloxifene, or newer drugs that specifically target bone components, such as romosozumab, have shown a beneficial effect against osteoporosis, but they often have moderate to severe side effects because estrogens are molecules with a wide range of physiological functions and receptors in many types of body tissues.
Another point to consider is that the skeleton acts as a natural reservoir for many minerals , with calcium, phosphorus, and magnesium as the main depositors. Therefore, there is a continuous exchange of ions with the body that depends largely on diet. A diet low in any of these three essential minerals will cause osteoclasts to overactivate in order to make them available to the rest of the body. A balanced diet rich in these minerals, while generally beneficial for the skeleton, may not be sufficient on its own if other molecules important for proper metabolism are not also ingested, such as vitamins D3 and K2, crucial for calcium absorption by the intestine and its fixation in bones, or the amino acid glycine, a fundamental component of collagen and one of the body's most demanded molecules, which is almost always in nutritional deficiency. Nutritional supplementation can help improve these processes, but in cases like magnesium, not all formulations are equally effective. In short, you can't build a house without bricks.
So, how can soy help us with osteoporosis?
And this is where we need to talk about soy, or more precisely , soy isoflavones . Isoflavones are phytoestrogens , plant compounds whose chemical structure is so similar to estrogens that they actually bind to their receptors and exert physiological effects through them . Some, like genistein and daidzein, have shown diverse therapeutic potential for coagulation disorders, hypercholesterolemia, and some types of cancer, and, of course, as estrogen replacement therapy for menopause and osteoporosis. Unfortunately, they also come with a price, often presenting some of the same side effects as medications like raloxifene.
In the late 1970s, research began into developing modified soy isoflavones that would possess the same beneficial properties with few or none of the side effects. The result was ipriflavone, a derivative of dadzein that does precisely that .
What is ipriflavone and where can you find it?
Ipriflavone is a semi-synthetic isoflavone; it does not occur naturally in soybeans, and the body cannot synthesize it on its own, so it must be consumed as a supplement . Like its natural precursors, it can bind to estrogen receptors, but—and this is important—it does so with a much higher affinity for the estrogen receptor type β (ER-β), the most abundant receptor in bone, which causes it to concentrate its activity there. Furthermore, although it binds to the receptor, it has no estrogenic activity, and in fact, it appears to enhance the activity of the most common estrogen replacement therapies by inducing an increase in the expression of that same ER-β receptor.
In vitro studies have shown that ipriflavone binding to ER-β helps slow the functional maturation of osteoclasts, thereby reducing bone resorption. Simultaneously, it promotes osteogenesis by facilitating the action of vitamin D on osteoblasts in two ways: 1) by stimulating the synthesis of the active metabolite 25-hydroxyvitamin D, and 2) by increasing the expression of the cellular receptor for vitamin D. This increases the absorption of calcium, making it available for bone formation.
Clinically, its action translates into improved bone quality. Clinical studies demonstrate that administering ipriflavone at doses of 300 to 600 milligrams daily improves bone mineral density , increases blood calcium levels, and decreases resorption markers in postmenopausal women with osteoporosis, contributing to a reduction in some typical menopausal symptoms such as hot flashes and bone pain, and an overall improvement in the patient's quality of life. So we can all walk with our heads held high.

Figures:
1. Figure 1: Common symptoms of osteoporosis and osteopathology
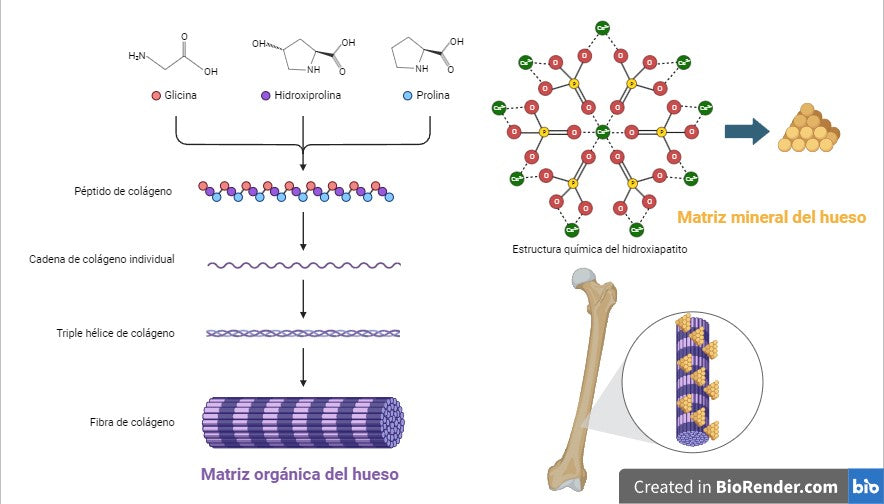
2. Figure 2: representation of the organic matrix and the mineral matrix of bone.
Collagen peptides, rich in glycine, hydroxyproline, and proline, associate in increasingly complex ways into chains, triple helices, and collagen fibers, creating the organic framework of bone. Hydroxyapatite crystals, containing calcium phosphate, are deposited on the collagen, giving bone its hardness. Ca2+: calcium; O: oxygen; P: phosphorus.
3. Action of ipriflavone on bone remodeling.
Ipriflavone is absorbed by the small intestine and binds to estrogen receptor β in bone. In osteoblasts, it facilitates the conversion of vitamin D to 1,25(OH)₂D, its active form, and increases the expression of its receptor. Furthermore, it increases the expression of ER-β and promotes the release of the protein osteoprotegerin, which slows the functional maturation of osteoclasts and decreases bone resorption. Ipr: ipriflavone; ER-β: estrogen receptor β; OPG: osteoprotegerin; Vit D: vitamin D.
References:
(Hooshiar et al, 2022)
(Park and Weaver, 2012)
(Hu et al, 2020)
(Zhang et al, 2010; Vitale el at, 2018).